


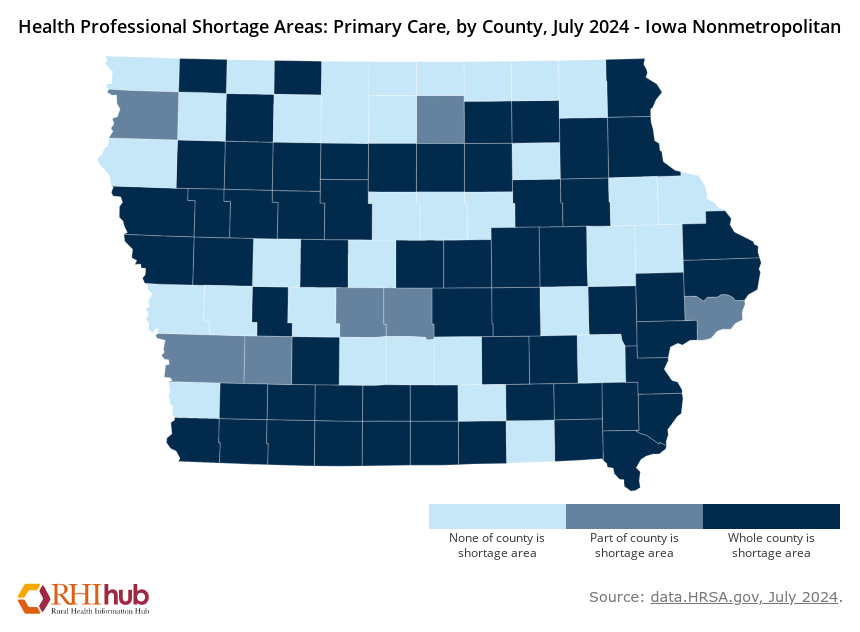
Iowa doesn’t have enough doctors. Over 2/3rds of Iowa’s 99 counties are experiencing a shortage of primary care doctors. The burden of this shortage has been predominantly borne by Iowans in rural areas. However, even Johnson county, home of the University of Iowa, one of the top medical universities in the country, is experiencing a shortage of primary care providers as well. Medical schools aren’t producing doctors at a fast enough rate to keep pace with increasing population.
The federal government has recognized this and has attempted to address the rising shortage for decades. More recently the Biden administration has implemented multiple programs including investing in primary care facilities, and loan forgiveness for doctors who practice in rural and designated crisis counties. The programs have totaled more than a billion dollars yet haven’t had any large or noticeable impact on the shrinking pool of available doctors. This crisis has been exacerbated by the COVID-19 pandemic which has caused many providers to burn out or retire early. In a report by the company Definitive Healthcare, more than 60% of doctors nationwide said their workload has increased since the pandemic, and between 2021 and 2022 more then 70,000 or 6% of physicians left the field.
There’s more behind this provider shortage then just burnout. People aged 65 and older are the fastest growing cohort and by 2030 nearly 80 million Americans will be in that category. On the supply side, young doctors and students are finding less incentive to become physicians. The pay and labor gap between physicians and other specializations that require just a few more years of education has caused many doctors to reject family medicine in favor of more specialized fields that come with higher pay and less workload.
A common culprit for the pay discrepancy between physicians and specialized fields falls on the RUC, a body of doctors that advises insurance companies and the federal government on how medical procedures should be priced. The RUC routinely rates general care procedures at a significantly lower cost than more specialized care, meaning doctors in general care get lower compensation from insurance for their work. In response to this market failure, nurses and physician assistants have filled the gap.

Between 2013 and 2019 the portion of healthcare visits handled by nurses and physician assistants nearly doubled, and according to the National Institutes of Health, “The proportion of visits delivered by nurse practitioners and physician assistants in the USA is increasing rapidly and now accounts for a quarter of all healthcare visits.” The trend of non-physicians filling the role of primary care has only grown since the pandemic, and continues to be one of the ways healthcare providers are attempting to meet demand with rising overhead costs and a shrinking pool of doctors. This practice has been touted as providing equal care while cutting costs by 25%.
Amy Sheaffer, President of A-1 Medical Staffing in Iowa has been in the field for over 20 years and says this isn’t the first time there’s been a shift in nurse’s responsibilities. “During World War I, the Red Cross created a volunteer nurse aid program as many nurses became overworked and tired. In the late 1960s, the physician assistant position was created as there was a shortage of primary care physicians due to access to healthcare and insurance increasing,” Sheaffer describes.
She says what she is seeing today with many doctors leaving the medical field is nothing like we’ve seen throughout history. Sheaffer notes though that many nurses are altering their roles and how they approach their job to fill in some of those gaps. “Nurses are reconsidering their priorities for a better work life balance and choosing flexible work opportunities. We are also seeing many trying to further their education to practice advanced nursing. This allows them to be properly compensated and assist in reducing the physician shortage by filling the primary care gap,” she said.
She also notes that as the healthcare landscape evolves, so do the roles within it. The increasing complexity of insurance policies and hospital billing has placed a heavier burden on medical staff, requiring more administrative oversight than ever before. Just as past workforce shortages led to the creation of new roles, today’s challenges in reimbursement and claims processing have given rise to specialized professionals who focus on Denial Management. These experts work to ensure that hospitals and clinics receive proper payment for services rendered, reducing financial strain on both providers and patients.
While this shift in roles has cut costs, it has pushed much of that onto lower paid and overworked nurses and physician assistants. Consumers and lawmakers worry this trend may lead to a weakening in the doctor-patient relationship and worsen health outcomes for patients. Some worry that this will lead to a healthcare gap between people in different economic classes, with the wealthy being able to retain a personal physician, while those with less money will have to deal with an incongruent, rotating cast of doctors for routine checkups. So far though, data suggests that outside of emergency or specialty care situations, nurses and physician assistants have similar patient outcomes to traditional family doctors.
Stay tuned in with KRUI
Programming features, updates, special events, and more delivered right to you